

Presentation:
Jane, a 64 year old lady called the clinic asking for an appointment. She’d been referred to us by her son and daughter-in-law. He had undergone successful treatment of low back and neck pain, she had successful management of severe lumbo-sacral pain, knee and hip pain.
Symptoms:
Jane’s chief complaint was a one month history of sudden onset Right sciatica extending from her buttock to the sole of her foot. Nothing seemed to make the pain either better or worse – it was constant and unrelenting. There was no Valsalva sign and no indication of Cauda Equina syndrome.
She had been diagnosed as having a “sciatic nerve problem” and treated unsuccessfully by an Osteopath.
Jane was also suffering from Right anterior knee pain. This had been present for approximately 6 months, was of sudden onset, unknown etiology, worsened by descending stairs and relieved by elevating her leg.
She had been previously diagnosed as having a “slipped patella” and treated by an Osteopath without success.
History:
While Jane had not suffered any previous major falls, fractures, dislocations, car accidents or loss of consciousness, she did have an extensive medical and surgical history.
She had undergone:
Tonsillectomy at 8yo
Vaginal cyst removal D&C and tubal ligation in 1994
Cholecystectomy in 2001
Abdominoplasty in 2003
CSF leak repair following surgery for a Sphenoid Meningeoencephalocele in 2007
Insertion of a pressure monitor for the Sphenoid Meningeoencephalocele later in 2007
Hiatus Hernia repair in 2008
Left Post Facial Craniotomy and MVD (Janetta procedure) of the Trigeminal nerve in 2012
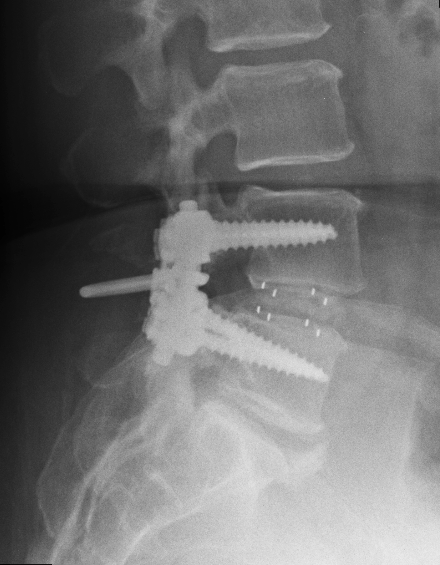
Surgical decompression and fusion of L4/5 in 2014
She was taking:
Lyrica 150mg morning and night
Coversil Plus 1.25mg+4mg
Examination:
Jane was quite short in stature and in her own words, “a little overweight”.
Orthopaedic:
Cervical ranges of motion were:
Flexion – 50° – no pain
Extension – 40°- no pain
Left Rotation – 60°- no pain
Right Rotation – 60°- no pain
Left Lateral Flexion – 20°- no pain
Right Lateral Flexion – 20°- no pain
Lumbar ranges of motion were:
Flexion – 60° – no pain
Extension – 10°- no pain
Left Rotation – 10°- no pain
Right Rotation – 10°- no pain
Left Lateral Flexion – 10°- no pain
Right Lateral Flexion – 10°- no pain
SLR was normal on the Left, but produced some pain and pulling into the gluteals at 40° on the Right.
Patrick FABER was strongly positive bilaterally with localised deep pain around the posterior greater trochanters.
Supported Adams, Cervical Compression and Maigne’s were all normal.
Examination of the right knee revealed increased lateral mobility across the tibial plateau and palpable-audible fine crepitus behind the patella on active flexion/extension.
Neurological:
All tendon reflexes were 2+
All cervical myotomes were 5+
All lumbo-sacral myotomes were 5+ except Right Hamstring, Glute Max & Gastrocnemius – 4+
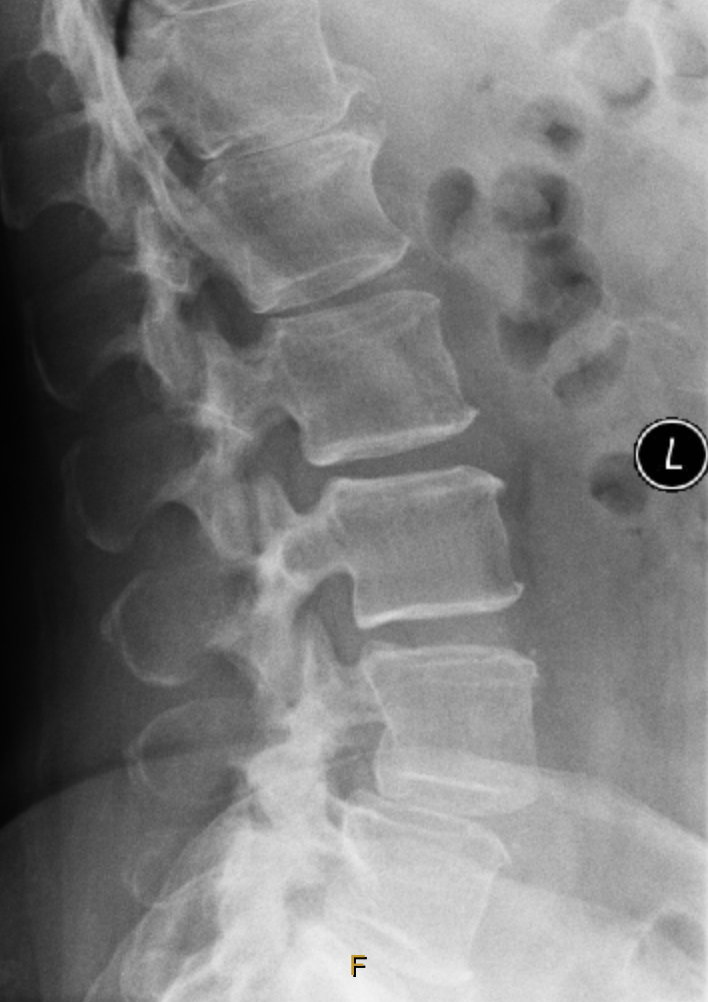
Images supplied by Patient – 17/12/2013
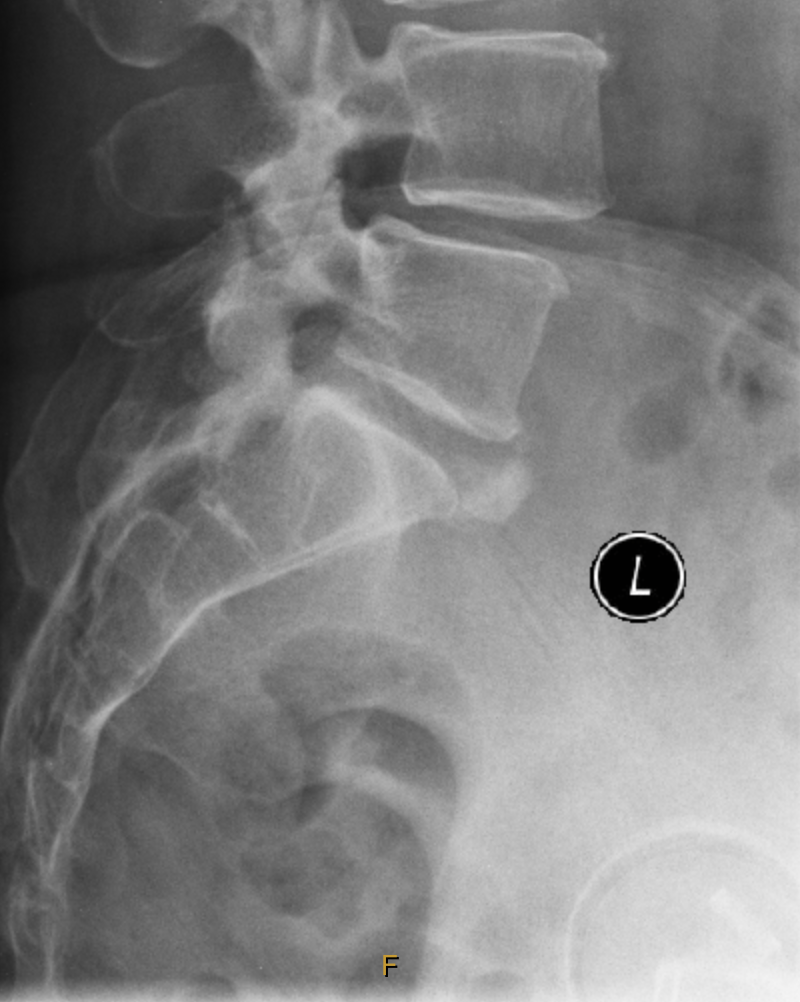
Images supplied by Patient – 24/04/2014

If You Have A Differential Diagnosis or Diagnoses, What Is It (or They)?
What Is Your Provisional Diagnosis?
What Further Tests (if any) Would You Do?
Is This A Chiropractic Case?